Introduction to implant placement in the mandible
An ideal alveolar ridge with adequate bone height and width is essential for successful dental rehabilitation. One of the most difficult surgical challenges for the implant surgery is severe resorption of the posterior mandible processes 1. The knowledge of the intra-osseous course of inferior alveolar nerve and vessels is mandatory for placing an implant in the body of the mandible. Damage to the inferior alveolar nerve can lead to motor and sensory abnormalities. So, the intra-osseous distribution of the inferior alveolar nerve is important in making an accurate pre-operative planning for the placement of mandibular implants 2. In an atrophic mandible, implant placement can be done in two ways, One, by increasing the bone level above the inferior alveolar canal by use of autogenous bone grafting, allografts, xenogeneic, or alloplastic materials with or without guided bone regeneration and distraction osteogenesis 3. Another method is by nerve lateralization 4. It carries a risk of epineural damage or ischemic stretching.
Anatomy of mandibular nerve
Mandibular nerve is a branch of the trigeminal nerve. Before we read in detail about the mandibular nerve and inferior alveolar nerve, let us discuss briefly the trigeminal nerve.
The trigeminal nerve is the largest of all the cranial nerves. It is a mixed nerve providing sensory supply to the face, the greater part of the scalp, the teeth, the nasal and oral cavity, the dura mater, the blood vessels of the cerebrum and motor supply to the muscles of mastication, mylohyoid and the anterior belly of digastric. It originates from the brainstem at the lateral surface of the pons, near its upper border, by a smaller motor and a larger sensory root. It exists the brain entering the trigeminal ganglion or Gasserian ganglion, where it gets divided into three major branches. The upper branch of the trigeminal nerve is the ophthalmic nerve (V1). It passes forward in the lateral wall of the cavernous sinus and gains access to the orbit via the superior orbital fissure. The middle branch is the maxillary nerve (V2). Maxillary division exits the middle cranial fossa through foramen rotundum and enters into the pterygopalatine fossa where it gives off several branches for the ……….Contents available in the book………..Contents available in the book………..Contents available in the book………..Contents available in the book………..Contents available in the book…….
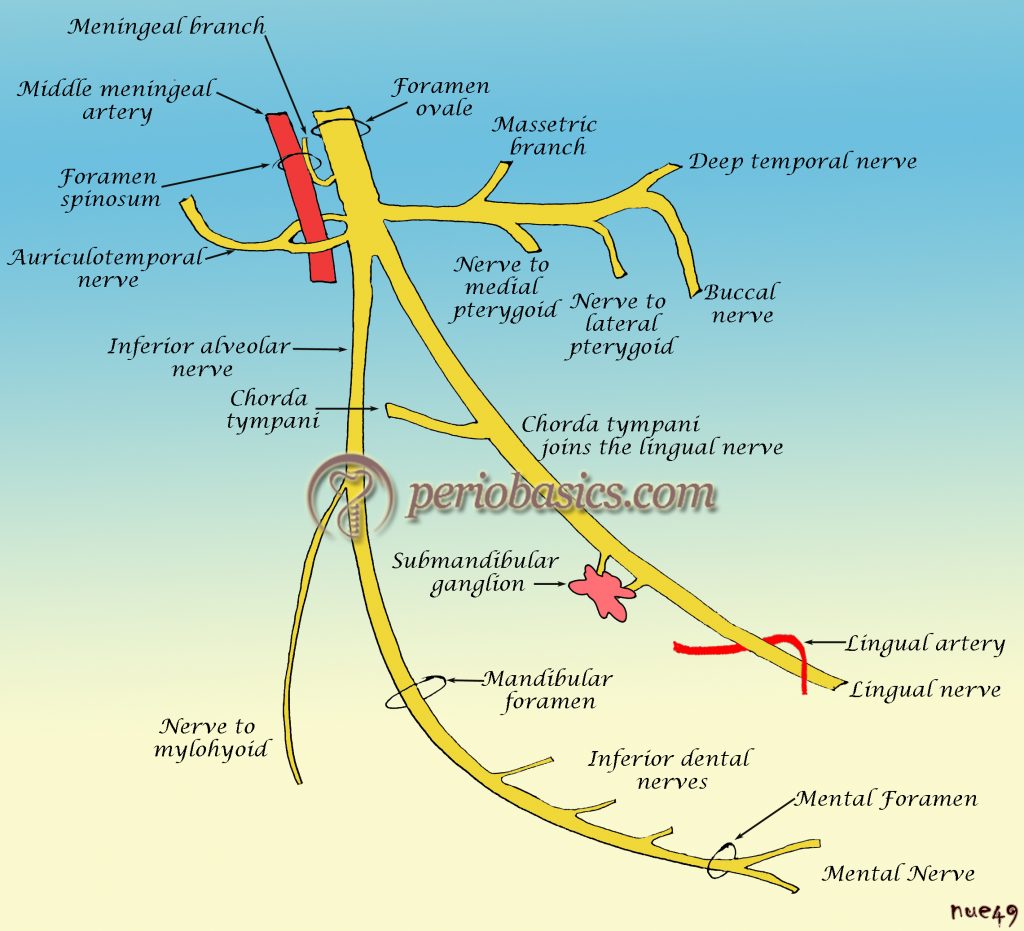
The mandibular nerve is the largest branch of the trigeminal nerve. As already stated it contains both afferent and efferent fibres. It leaves the skull through the foramen ovale and enters the infratemporal fossa where medial to the lateral pterygoid muscle it divides into a smaller anterior trunk and a larger posterior trunk.
Anterior trunk of mandibular nerve
This division presents a larger amount of motor nerve fibers than sensory ones. It gives the following branches:
Masseteric nerve:
It is responsible for the motor innervation of the masseter and probably for sending tiny branches that supply the temporomandibular joint (TMJ).
Nerves to the lateral and medial pterygoid:
These nerves also arise from the anterior division of the mandibular nerve and they supply the motor innervation of these muscles. Both of these muscles play a vital role during masticatory cycle.
Deep temporal nerves:
In a number of two, one anterior and one posterior, they supply the anterior and posterior parts of the temporal muscle, respectively.
Buccal nerve:
Although pertaining to the anterior division, it bears sensitive nerve fibers. It supplies the cheek skin and mucous membrane, except that of the region supplied by the posterior superior alveolar branches from the maxillary nerve.
Posterior trunk of mandibular nerve
This division has a larger amount of sensory nerve fibers than the motor ones. It has following branches,
Auriculotemporal nerve:
It usually has 2 roots, arising from the posterior division of the mandibular nerve. It encircles the middle meningeal artery and runs posteriorly passing between the sphenomandibular ligament and the neck of the mandible. It carries somatosensory and secretomotor fibers of the mandibular nerve and the glossopharyngeal nerve.
Lingual nerve:
The lingual nerve lies between ramus and medial pterygoid, within the pterygomandibular raphe. It passes inferior and medial to the mandibular 3rd molar alveolus. It provides sensation to anterior 2/3rds of the tongue, lingual gingiva, floor of mouth mucosa, and gustation (chorda tympani).
Nerve to mylohyoid:
The mylohyoid nerve branches from the inferior alveolar nerve before it enters the mandibular canal. It provides motor nerve fibers to these muscles and sensitive nerve fibers to the neighboring skin.
Inferior alveolar nerve:
This branch enters the mandibular foramen. It supplies the mandibular teeth and the associated periodontium. It is a very important nerve as far as implantology is concerned. Let us now, discuss this nerve in detail.
Inferior alveolar neurovascular bundle
The mandibular nerve enters the mandible through the mandibular foramen on the medial surface of the ascending mandibular ramus. After passing through the mandibular foramen, the nerve is called the inferior alveolar nerve. Within the mandibular canal, the inferior alveolar nerve runs forwards in company with the inferior alveolar artery, vein, and lymphatic vessels and together they are called as inferior alveolar neurovascular bundle. The inferior alveolar nerve runs in the mandibular canal as a single trunk, giving branches for molar and premolar teeth. In the premolar region, the nerve gives the incisive nerve for premolar, canine and incisor teeth and the mental nerve. The buccolingual positioning of the inferior alveolar nerve has been studied well. In a recent study, Kim et al. (2009) 10 classified the buccolingual location of the inferior alveolar nerve into 3 types,
In most of the cases (70%), the inferior alveolar nerve canal follows the lingual cortical plate of the mandibular ramus and body. In 15% of cases, the inferior alveolar nerve canal is located in the middle of the mandibular ramus posterior to the second molar. It then runs lingually to follow the lingual plate. In 15% of cases, the inferior alveolar nerve canal is located ……….Contents available in the book………..Contents available in the book………..Contents available in the book………..Contents available in the book………..Contents available in the book…….

Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.
India Users:
International Users:
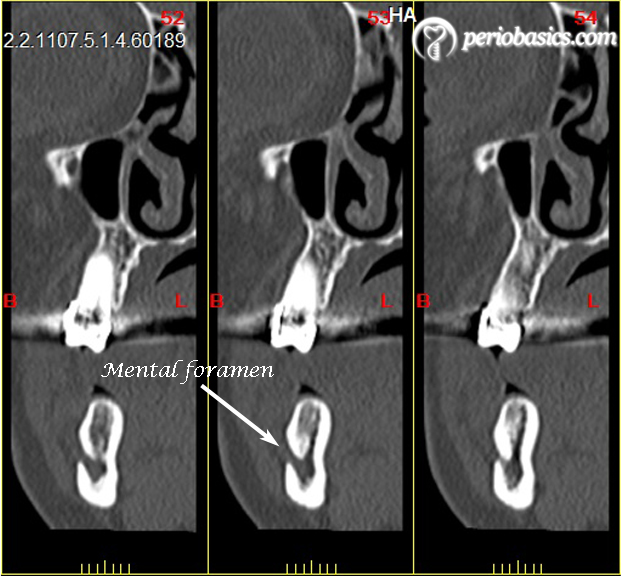
Peculiarities of mental foramen (clinical anatomy)
One of the most challenged regions for implantation in the mandible is mental foramen region. This is because there are many variations with regards to the size, shape, location and direction of the opening of the mental foramen. The shape of mental foramen can be round or oval: diameter ranges from 2.5 to 5.5 mm 11-14. The outer end of the mental canal occupies a higher and more posterior plane than its inner end. One study found different shapes of the mental foramen in the mandibles of Zimbabwean subjects: round in 14 of 32 (43.8%) mandibles and oval in 18 of 32 (56.3%) jaws 15. The average size of the mental foramen has been estimated to be 3.47 mm (range: 2.5 to 5.5 mm) in height and 3.59 mm (range: 2 to 5.5 mm) in width 16.
The mental foramen is usually located near the apex of the second mandibular premolar or between the apices of the premolars. However, anatomical variations occur concerning the mental foramen’s location 17, 18. After extraction of teeth, the resorption of alveolar bone takes place because of which mental foramen comes closer to the alveolar crest 13, 19.
In extreme situations, the mental foramen and mandibular canal can be adjacent to the crest of the alveolar ridge 20. Mental foramen is usually located more coronal than the mandibular canal. It has also been reported that more than one mental foramen may be present 17, 18. One study assessed the frequency of accessory mental foramina in skulls in four population groups which included American Whites (frequency of accessory mental foramen = 1.4%); Asian Indians (frequency of accessory mental foramen = 1.5%); African Americans frequency of accessory mental foramen = 5.7%); and pre-Columbian Nazca Indians (frequency of accessory mental foramen = 9.0%) 18. The most common emergence pattern of the mental foramen of the mental canal is usually in a posterior direction. However, a study done on Zimbabwean subjects frequently detected a right-angled exit path 15.

The section of the nerve in front of the mental foramen and just before its ramification to the incisive nerve can be defined as the anterior loop of the inferior alveolar nerve. Although the length of the anterior component of the mental canal is not given, it is implied that it is consistently present. During implant placement, any violation of this loop may result in neurosensory disturbances in the area of the lower lip and chin. The radiographic examination provides the clinician, the information about mandibular canal and mental foramen. But, the ability of conventional two-dimensional ……….Contents available in the book………..Contents available in the book………..Contents available in the book………..Contents available in the book………..Contents available in the book…….
To avoid nerve injury, it is desired to place an implant, leaving a 2-mm safety zone above the nerve and if the implant is placed anterior to the mental foramen, then the distal surface of the implant should be ≥2 mm mesial to the mental foramen 23.
Nerve injuries
Seddon (1943) 24 described three types of nerve injury-neurapraxia, axonotmesis, and neurotmesis based on the severity of tissue injury, the prognosis for recovery, and time for recovery.
Neurapraxia:
It is conduction block resulting from a mild insult to the nerve trunk. There is no axonal degeneration, and sensory recovery is complete and occurs in a matter of hours to several days. The sensory deficit is usually mild and characterized by a paresthesia, with some stimulus detection but poor discrimination and disturbed stimulus interpretation.
Axonotmesis:
It is a more severe nerve injury as compared to neurapraxia. Afferent fibers undergo degeneration, but the nerve trunk is grossly intact with variable degrees of tissue injury. Sensory recovery is good but incomplete. The time course for sensory recovery depends on the rate of axonal regeneration and usually takes several months. The sensory deficit is characterized by a severe paresthesia.
Neurotmesis:
This is the most severe kind of nerve injury where complete disruption of the nerve takes place. Sensory recovery is not expected except when the nerve courses through a canal like the mandibular canal. The sensory deficit is characterized by anesthesia.
Healing following the nerve injury
After an injury, the nerve tries to repair itself by sprouting regenerating nerve units. These regenerating nerve units, then try to grow down the nerve to re-innervate muscle or skin. The nerves regenerate at a rate of 1 inch per month. During regeneration of the nerve, if the ……….Contents available in the book………..Contents available in the book………..Contents available in the book………..Contents available in the book………..Contents available in the book…….
Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.
India Users:
International Users:
Inferior alveolar nerve lateralization
In many cases, there is an insufficient bone for implant placement in the posterior mandibular region. The inferior alveolar never is the limiting factor, which should not be injured during the surgical procedure. To overcome this problem the inferior alveolar nerve lateralization procedure has been described. This surgical procedure involves the surgical exposure of the inferior alveolar nerve, releasing it from the inferior alveolar canal and placing it on the lateral aspect of the implant after the implant has been inserted up to the desired level in the bone.
Surgical procedure:
In 1987, Jensen and Nock 25 were the first to publish this technique developed for the translocation of the mental foramen. A detailed description of the nerve lateralization procedure has been given in “Clinical procedure for dental implant placement”. This procedure is associated with the risk of temporary or even permanent irritation of the nerve, which may lead to anesthesia, hypesthesia or paresthesia. Various studies have been done to investigate the resolution of sensory complications which demonstrate variable results 26, 27. Because of the variability in results reported, further investigations of the long-term neurosensory outcome of this procedure are needed. The patient must be told about the complications before attempting the procedure. Six to eight weeks of lasting paresthesia of the mental nerve and the possibility of a permanent paresthesia should be told to the patient.
Conclusion
The in-depth knowledge of the mandibular nerve is essential during placement of implants in the mandibular posterior area. Although we have various radiographic methods to identify the course of the mandibular nerve, but care must always be taken during implant placement because all imaging techniques have their own limitations. Inferior alveolar nerve transposition is a useful adjunct for managing the atrophic posterior mandible with dental implants. CT scans are necessary to accurately locate the mandibular canal before undertaking nerve repositioning for implant placement, and it is important that only well-experienced surgeons perform this surgery. Because of the benefits of the inferior alveolar nerve lateralization procedure, it is becoming more and more popular procedure. Lastly, it is the experience and efficiency of the operator which plays an important role in the overall success of this treatment.
References
References are available in the hard-copy of the website.
Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.